Food is Medicine: A movement reshaping healthcare and the future of farming

What we eat shapes how we feel, how we heal, and how long we can enjoy health. In this guest article, Zuzanna Zielińska and Anne van de Peppel – co-founders of HarvestCare and frontrunners of the Dutch Food is Medicine movement – explore what it truly means to bring this wisdom into today’s healthcare systems.
Modern healthcare has achieved extraordinary things. Advances in pharmaceutical science, surgery, and medical technology have helped humanity overcome diseases that once claimed millions of lives. And yet we now face a different kind of epidemic – one driven not by viruses or bacteria, but largely by what we eat. Chronic conditions like type 2 diabetes, cardiovascular disease, and obesity are among the leading causes of death and disability worldwide, and they are deeply linked to diet. This raises an important question: can medicine alone be the answer, when the root cause so often lies on our plates?
A growing movement of researchers, clinicians, farmers, and policymakers is challenging that status quo. They unite under the name ‘Food is Medicine’ (sometimes also referred to as ‘Food as Medicine’) – a rapidly growing scientific field and policy movement with dedicated funding, peer-reviewed research, and practitioners working on every continent to integrate nutrition into clinical care. Hundreds of thousands of patients are already using food-based interventions to prevent and manage chronic conditions. This article aims to paint a clear picture of what that movement looks like – and why it matters for the future of food and farming in Europe.
A note on sources: the Food is Medicine movement is most advanced in the United States, and much of the available scientific literature currently reflects that context. As the movement grows globally, more evidence from local contexts will become available. For now, this article draws primarily on US sources, while connecting their relevance to the Dutch and European situation.
Uitgelichte quote
We now face a different kind of epidemic - one driven not by viruses or bacteria, but largely by what we eat
 “Hundreds of thousands of patients are already using food-based interventions to prevent and manage chronic conditions.” Photographer: Ruben Hamelink at Mensa Mensa
“Hundreds of thousands of patients are already using food-based interventions to prevent and manage chronic conditions.” Photographer: Ruben Hamelink at Mensa Mensa
 “Can medicine alone be the answer, when the root cause so often lies on our plates.” Photographer: Ruben Hamelink at Mensa Mensa
“Can medicine alone be the answer, when the root cause so often lies on our plates.” Photographer: Ruben Hamelink at Mensa Mensa
What is ‘Food is Medicine’?
The phrase ‘Food is Medicine’ is often misunderstood as a general call for healthy eating or a nutritional intervention – sometimes reduced to a wellness lifestyle trend. The Tufts University Food is Medicine Institute defines it as: interventions reflect the critical link between nutrition and health, integrated into healthcare delivery, providing medically tailored meals, groceries, and produce to support disease management, in combination with nutrition and culinary education, as part of a patient’s healthcare treatment plan (Tufts University, 2025).
To put it simply: Food is Medicine does not merely recommend that patients eat better. It ensures that the food patients need to improve their health is actively provided as part of their care – much as medication is prescribed and dispensed through the healthcare system. At its core, the movement is also advocating for health equity. Diet-related chronic diseases disproportionately affect people living with food insecurity and low incomes, who often face structural barriers to accessing food that could support their health. Food is Medicine interventions are designed to ensure that access to nutritious food is not a privilege, but a meaningful component of healthcare.
Uitgelichte quote
Can medicine alone be the answer, when the root cause so often lies on our plates?
Within the movement, there are three main clinical interventions that are the subject of most research:
Medically Tailored Meals (MTM) are home-delivered meals designed by a registered dietitian specifically for an individual’s medical condition. They are intended for patients who are too ill to shop or cook for themselves, and tailored to conditions such as heart failure, cancer, diabetes, or chronic kidney disease.
Medically Tailored Groceries (MTG) are packages of nutritionally appropriate groceries designed for a patient’s specific dietary needs. They allow patients to continue preparing their own food at home, supporting both practical independence and the development of lasting dietary habits.
Produce Prescriptions (PRx) are the broadest and most scalable intervention: clinicians prescribe fruits and vegetables — through vouchers, subsidised boxes, or direct partnerships with local food providers — to patients with diet-related conditions or food insecurity. In the Netherlands, HarvestCare is among the first organisations implementing this model through its Voedsel op Recept programme in the province of South Holland.
Alongside these three clinical interventions, population-level food policies and nutrition security programmes also play an important complementary role — but they fall outside the scope of this article.
Uitgelichte quote
It emerged from communities organising around a basic, urgent need
 “Food is Medicine interventions are designed to ensure that access to nutritious food is not a privilege, but a meaningful component of healthcare.” Photographer: Ruben Hamelink at Mensa Mensa
“Food is Medicine interventions are designed to ensure that access to nutritious food is not a privilege, but a meaningful component of healthcare.” Photographer: Ruben Hamelink at Mensa Mensa
 “It ensures that the food patients need to improve their health is actively provided as part of their care.” Photographer: Ruben Hamelink at Mensa Mensa
“It ensures that the food patients need to improve their health is actively provided as part of their care.” Photographer: Ruben Hamelink at Mensa Mensa
A brief history of the movement
Despite hundreds of published papers and a growing body of clinical evidence, the Food is Medicine movement did not originate in research institutions or academic theory. It emerged from communities organising around a basic, urgent need: access to healthy food for people who were sick, but faced structural barriers to accessing food that could help them heal.
Some of the first produce prescription programmes in the United States grew directly from farmers’ markets and community-supported agriculture (CSA) schemes – local food networks that were already meeting community health needs informally, long before healthcare institutions took notice. Over time, researchers and health professionals recognised the value of these interventions and began to research the evidence and create institutional frameworks to support them at scale.
The moment most often cited as the movement’s turning point is the HIV/AIDS epidemic of the 1980s. As the crisis devastated communities across American cities, volunteer organisations in Boston, New York, and San Francisco began delivering medically tailored meals to people living with HIV, many too ill to care for themselves. At that time, these initiatives were not part of the healthcare system, but acts of community solidarity. In 1990, the Ryan White CARE Act formally recognised the role of nutrition in HIV management and created federal funding for nutrition services. By the late 1990s, most of these pioneering organisations had expanded to serve people living with many other serious illnesses (Aspen Institute, 2024; Volpp et al., 2023).
Uitgelichte quote
Diet-related chronic diseases disproportionately affect people living with food insecurity and low incomes
 “The most common target populations in existing research are people living with type 2 diabetes, cardiovascular disease, and chronic kidney disease.” Photographer: Gabriela Hengeveld
“The most common target populations in existing research are people living with type 2 diabetes, cardiovascular disease, and chronic kidney disease.” Photographer: Gabriela Hengeveld
 “Combining food provision with culinary education and behavioural support outperforms food provision alone.” Photographer: Gabriela Hengeveld
“Combining food provision with culinary education and behavioural support outperforms food provision alone.” Photographer: Gabriela Hengeveld
In 2010–2013, several nonprofits coalesced into the Food is Medicine Coalition. That same year, the Affordable Care Act created new pathways for states to pilot innovative care models, enabling food-based interventions to be tested within healthcare financing structures. A further significant milestone came in 2014, when the US Congress passed the Gus Schumacher Nutrition Incentive Program (GusNIP) as part of the Farm Bill, administered by the Department of Agriculture. It was a meaningful step for the agricultural sector to formally recognise its stake in public health and commit dedicated federal funds to develop prescription programmes for low-income populations at risk of diet-related disease (Aspen Institute, 2024).
The momentum continued to build, as in 2022, the Biden-Harris White House Conference on Hunger, Nutrition and Health mobilised more than $8 billion in public and private commitments across a range of hunger and nutrition programmes, with specific recommendations to expand FIM access in Medicare and Medicaid (Aspen Institute, 2024). In 2023, the American Heart Association and the Rockefeller Foundation jointly committed $250 million over 10 years to a Food is Medicine Research Initiative, with a strategic objective of unlocking national policy support (Aspen Institute, 2024; Schwartz et al., 2025).
Uitgelichte quote
Benefits to quality of life and mental health are also well documented
What does science say?
The scientific evidence examining the impact of ‘Food is Medicine’ has grown substantially over the past decade. What began as small-scale pilots and quasi-experimental studies has matured considerably. Currently, well over 250 scientific papers have been published on FIM interventions, and the field has now reached the level of systematic reviews of randomised controlled trials (Ridberg et al., 2025).
The most consistent findings from FIM interventions are improvements in diet quality (particularly increases in fruit and vegetable consumption) and meaningful reductions in food insecurity. Benefits to quality of life and mental health are also well documented, including reduced depressive symptoms, improved social connectedness, and reduced loneliness (Seligman et al., 2025; Ridberg et al., 2025).
When it comes to clinical outcomes, such as blood glucose levels, weight, and hospitalisation rates, the evidence is less consistent. Some trials show meaningful improvements; others do not reach statistical significance. This is partly a reflection of the complexity of measuring food’s long-term impact on health, and partly a methodological challenge. FIM programmes differ widely in the intensity and type of food provided, the duration of the intervention, and the populations served (Seligman et al., 2025; Downer et al., 2020).
The most common target populations in existing research are people living with type 2 diabetes, cardiovascular disease, and chronic kidney disease, often in combination with food insecurity. What the field broadly agrees on is that longer, more intensive programmes tend to show stronger effects, and that combining food provision with culinary education and behavioural support outperforms food provision alone. Several ongoing longer-term trials are expected to shed considerably more light on the durability and clinical significance of these outcomes in the coming years.
 “The movement is now working to structurally align its growing healthcare demand with agriculture that supports healthy soils, biodiversity, and the preservation of ecosystem services.” Photographer: On a hazy morning
“The movement is now working to structurally align its growing healthcare demand with agriculture that supports healthy soils, biodiversity, and the preservation of ecosystem services.” Photographer: On a hazy morning
Food is Medicine and the food system
Food is Medicine research is now expanding its scope to account for its impact on the food system – a dimension that was at the core of the first community-based Food is Medicine interventions. The movement is now working to structurally align its growing healthcare demand with agriculture that supports healthy soils, biodiversity, and the preservation of ecosystem services.
Food is Medicine, by creating structural demand within local, short-chain supply chains, offers a real and significant opportunity for small- and medium-sized local farmers. When healthcare systems procure nutritious food at scale for patients, the ripple effects on food production are considerable. FIM has the potential to reshape markets for agroecological food producers, shifting the economic incentives of food production away from a sole focus on yield per hectare toward metrics like nutritional density, ecological integrity, and local sourcing (Rahman et al., 2024).
The Rockefeller Foundation’s From Farm to FIM report provides concrete numbers. If FIM programmes were implemented at scale with a focus on local sourcing, they could support more than 316,000 jobs, generate over $45 billion in annual GDP growth, and deliver $5.6 billion in annual revenue for small and mid-sized family farms. For farmers navigating the financial precarity of transitioning to regenerative or organic practices, the reliable institutional demand created by FIM programmes could be transformative (Rockefeller Foundation, 2026).
This potential is particularly relevant for the Netherlands. The Dutch government has committed to increasing organic farmland to 15% of total agricultural area by 2030 – a target that currently sits at around 4%. Meeting it requires institutional demand: new, reliable markets that make the transition to organic or regenerative farming economically viable. Produce prescription programmes, embedded in healthcare, could create exactly that: a stable, healthcare-funded market for local, high-quality produce.
Uitgelichte quote
Several major US insurers now cover produce prescriptions or medically tailored groceries
How is Food is Medicine financed?
Funding for Food is Medicine programmes has historically been a patchwork, and this remains one of the movement’s central challenges. Most programmes rely on a blend of philanthropy, governmental grants at the federal, state, and municipal levels, research funding, and – increasingly – reimbursement from health insurers. The entry of insurers represents the most significant recent shift: several major US insurers now cover produce prescriptions or medically tailored groceries for patients with specific chronic conditions, and more than three-quarters of Medicare Advantage enrollees are in plans that offer some form of food benefit (Schwartz et al., 2025). This transition from philanthropy to structural healthcare financing is widely seen as the key to scaling the movement.
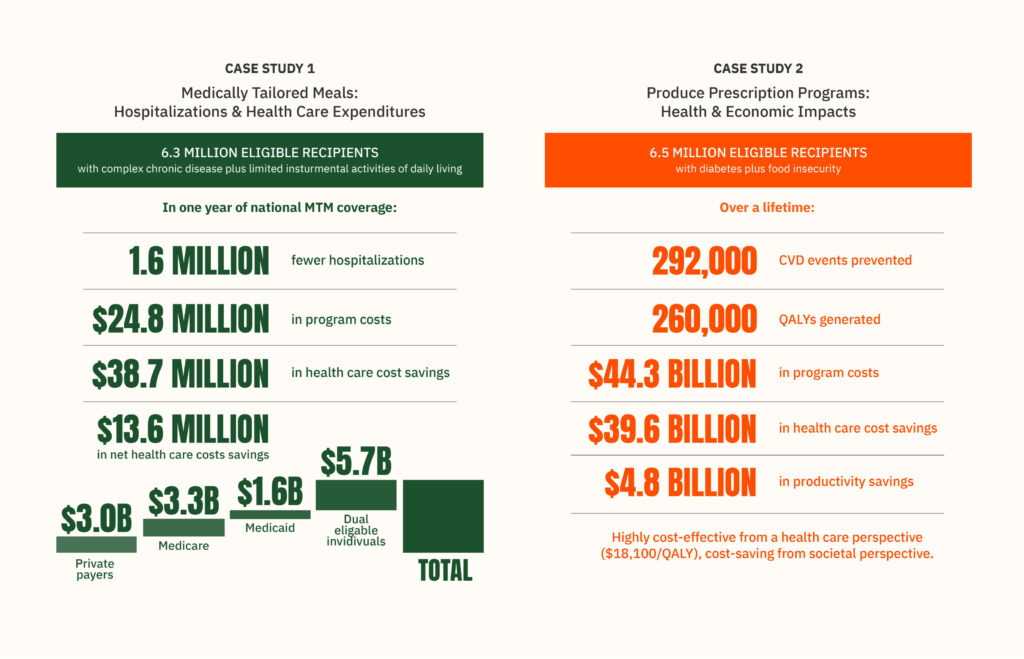
Modelling by Tufts University shows that population-wide coverage for patients with food insecurity and chronic diseases would yield meaningful reductions in hospitalisations and healthcare costs. It is worth noting that these projections were based on relatively modest programme costs, and more comprehensive programmes may require higher investment, but the direction of the finding is encouraging (Tufts University, 2023).
In the Netherlands, HarvestCare is exploring an additional financing pathway: an Agri-Health Outcome Payment Model, a blended-finance mechanism funded by the Province of Zuid-Holland and the European Union, in which private and public funders provide upfront capital and are repaid by healthcare institutions when agreed-upon health outcomes are achieved.
Uitgelichte quote
In the Netherlands, HarvestCare is exploring an additional financing pathway
 “Rewarding farmers for growing nutritious, regenerative and locally sourced food.” Photographer: Ruben Hamelink at Mensa Mensa
“Rewarding farmers for growing nutritious, regenerative and locally sourced food.” Photographer: Ruben Hamelink at Mensa Mensa
 “If agricultural policy incentives were aligned with Food is Medicine Goals, it could begin to shift agriculture towards producing food that feeds directly into healthcare pathways.” Photographer: Ruben Hamelink at Mensa Mensa
“If agricultural policy incentives were aligned with Food is Medicine Goals, it could begin to shift agriculture towards producing food that feeds directly into healthcare pathways.” Photographer: Ruben Hamelink at Mensa Mensa
In September 2025, a global convening hosted by the Rockefeller Foundation at its Bellagio Centre brought together participants from many countries across Africa, Asia, Europe, and the Americas. For the first time, this group worked toward a set of Global Food is Medicine Principles – foundational guidelines defining how Food is Medicine interventions should be integrated into healthcare systems globally, covering integration, equity, scientific rigour, and scalability (Rockefeller Foundation, 2025). Based on this gathering, a Global Food is Medicine Alliance has been formed, dedicated to accelerating implementation and evidence-building across regions. HarvestCare had the honour of becoming a founding member.
Uitgelichte quote
Every year, more than €700 billion is spent across the EU on managing chronic diseases
The European context
In the European Union, the conditions for building the FIM movement are both urgent and complex. Every year, more than €700 billion is spent across the EU on managing chronic diseases. In many cases, these are conditions that are preventable and, with the right interventions, even reversible. Despite the common sense of investing in prevention, the challenge of how to arrange and sustain such investments remains largely unsolved.
The diversity of European healthcare systems – each shaped by different national structures, insurance models, and regulatory frameworks – makes EU-wide adoption of Food is Medicine a real challenge. There is no single pathway that works in every country, and building evidence in local contexts will take time and major investment.
And yet there is a significant opportunity in how Europe currently funds both its farmers and its healthcare. The Common Agricultural Policy (CAP) allocates approximately €387 billion over seven years (2021–2027) to support farming across the continent. If CAP incentives were aligned with Food is Medicine goals – rewarding farmers for growing nutritious, regenerative, and locally sourced food – it could begin to shift agriculture toward producing food that feeds directly into healthcare pathways. If healthcare budgets were to allocate even a fraction of their spending to the provision of nutritious food, a real and stable demand for local, high-quality produce could follow. Both levers together could offer small and mid-scale farmers across Europe a market that rewards quality over quantity – while benefiting patients and relieving pressure on healthcare systems.
Across Europe, practitioners, researchers, and professionals passionate about the connection between farming and healthcare are beginning to build this movement in their own contexts. We hope that the Netherlands – with its commitment to regenerative agriculture transitions and its culture of innovation – will be a leading voice in the European Union on the implementation of Food is Medicine.
Would you like to dive deeper into Food is Medicine? HarvestCare and RHEA are organising the first European Food is Medicine and Agri-Health Summit, bringing together experts in medicine and its connection to regenerative farming, on the 19th and 20th of November in Amsterdam.
Interested in starting your own Food is Medicine project? Sign up for the pitch competition and stand a chance to win up to €10,000 to kick-start your idea.


